

Introduction: MM is an incurable disease with risk categorizations by cytogenetic abnormalities. Prognostic implications of chromosome translocation t(11;14)+ are important to inform development of biomarker-targeted therapies such as the B-cell lymphoma-2 (BCL-2) pathway inhibitors. This study aims to evaluate MM treatment (Tx) patterns and outcomes of t(11;14)+ compared with other cytogenetic cohorts in US routine clinical practice.
Methods: A retrospective observational cohort study of the Flatiron Health database, which comprises de-identified electronic health record-derived patient (pt)-level data from over 280 community and academic cancer clinics in the US. Pts aged ≥18 years who received a first-line (1L) induction Tx within ≤60 days of MM diagnosis from 1/1/2011 to 1/31/2020, and were not enrolled in a clinical trial were identified at the start of each Tx line (index date) and followed up (f/u) until 1/31/2020. Only cytogenetic results by fluorescence in situ hybridization (FISH) were used to stratify the cohort into: t(11;14)+; standard risk, excluding t(11;14)+ (SR); and high risk, (HR; del 17p, t(4;14), t(14;16), t(14;20), chromosome 1 abnormalities as a proxy for 1q gain; and t(11;14) where it co-occurs). Descriptive analyses of pt characteristics and Tx were conducted. Kaplan-Meier analyses were used to evaluate median time to next treatment (TTNT) and overall survival (OS) with log-rank test for significance. The cohort was stratified by age ≤70/>70 years (yrs) as a proxy for transplant eligibility.
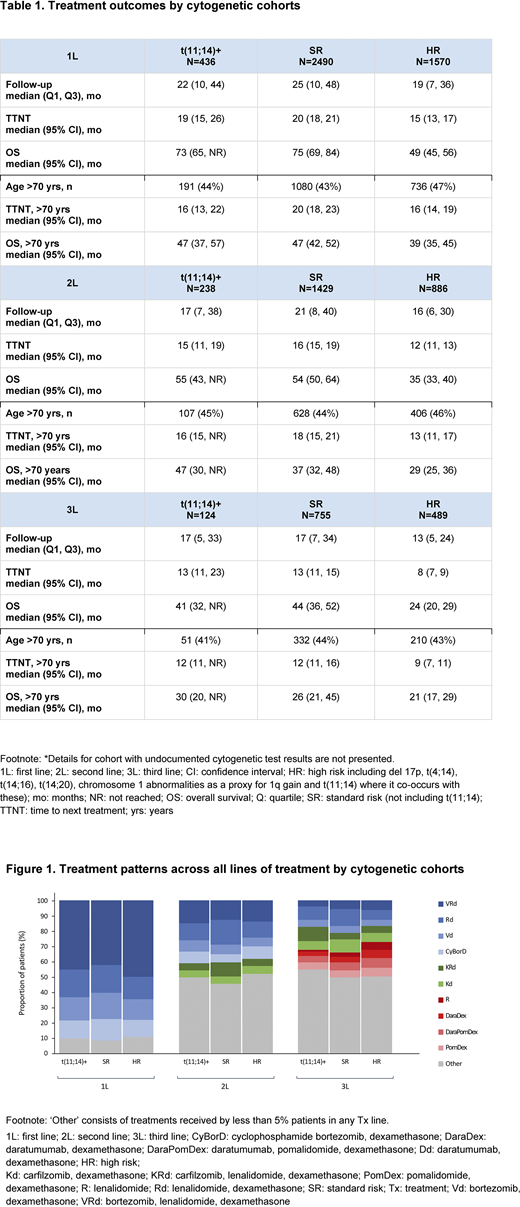
Results: Of 10,703 pts with MM in the database, 5982, 3059 and 1595 pts were eligible for 1L, second-line (2L), and third-line (3L) analysis, of which 76%, 84%, and 86%, respectively, had FISH test results before Tx initiation. 14% of pts with FISH test results were t(11;14)+, ~55% SR and ~35% HR. Included pts were predominately male (55%), ~90% treated in the community setting and ~16% African-American. Pts in the 3L cohort were younger at diagnosis with a median age (interquartile range) of 67 (59 ̶ 74) yrs compared with 69 (61 ̶ 76) yrs in both 1L and 2L. The 1L Tx pattern was consistent across cytogenetic cohorts with bortezomib (V), lenalidomide (R), dexamethasone (d) as the most common Tx (>42%). Together, VRd, Rd, Vd, and cyclophosphamide (Cy) in combination with Vd represented ≥90% of 1L Tx (Figure 1). Across 2L cytogenetic cohorts, the most common Tx regimens (≥25%) were VRd and Rd. The use of regimens containing carfilzomib (K) and daratumumab (D) was emerging in 2L: KRd in 8% of t(11;14)+ and HR and 5% in SR; Kd 5% in all groups; DRd in 4% of t(11;14)+ and 3% in SR and HR (Figure 1). 3L Tx pattern was fragmented with different Tx regimens. Rd was the most common 3L Tx option: 9% in t(11;14)+, 10% in SR and 7% in HR (Figure 1). Across all lines of Tx, t(11;14)+ had similar Tx outcomes to SR, and HR had poorest outcomes (Table 1). Pts TTNT shortened as they advanced to later lines of Tx (Table 1). Although TTNT did not differ by age across lines of Tx, OS was superior in pts <70 yrs across all 3 cytogenetic risk cohorts, especially in 1L where transplant in those ≤70 yrs vs >70 yrs at diagnosis was 44% vs 11% for t(11;14)+, 47% vs 10% for SR and 49% vs 9% for HR.
Conclusions: This study identified cytogenetic subgroups across 1L to 3L in a predominately community setting in the US. MM t(11;14)+ pts had similar 1L and 2L Tx patterns to SR and HR. Across all lines of Tx, the outcomes of t(11;14)+ and SR pts were comparable and better than HR pts. TTNT was reduced as pts advanced to later lines of Tx. Pts continuing to 3L Tx were younger at diagnosis, but there was not a clear-cut standard of care. While TTNT did not differ by age across lines of Tx, OS was superior in pts <70 yrs across all 3 cytogenetic risk cohorts. This study sets the benchmark for novel treatment options, such as BCL-2 pathway inhibitors, primarily wherever available biomarker-driven therapy is considered appropriate.
Atrash:Takeda, Amgen, Karyopharm, BMS, Sanofi, Cellactar, Janssen and Celgene: Honoraria; BMS, Jansen oncology, Sanofi: Speakers Bureau; Amgen, GSK, Karyopharm.: Research Funding. Flahavan:F. Hoffmann-La Roche: Current equity holder in publicly-traded company; Roche Products Ltd.: Current Employment. Xu:F. Hoffmann-La Roche Ltd: Current Employment, Other: All authors received support for third party writing assistance, furnished by Scott Battle, PhD, provided by F. Hoffmann-La Roche, Basel, Switzerland.. Ma:Genentech, Inc.: Current Employment, Current equity holder in publicly-traded company. Karve:AbbVie: Current Employment, Current equity holder in publicly-traded company. Hong:F. Hoffmann-La Roche: Current equity holder in publicly-traded company; Genentech, Inc.: Current Employment. Jirau-Lucca:Genentech, Inc.: Current Employment; AbbVie: Current equity holder in publicly-traded company; BMS: Current equity holder in publicly-traded company; Celgene: Divested equity in a private or publicly-traded company in the past 24 months. Nixon:Genentech, Inc.: Current Employment, Current equity holder in publicly-traded company; F. Hoffmann-La Roche: Current Employment, Current equity holder in publicly-traded company. Ailawadhi:Takeda: Honoraria; Pharmacyclics: Research Funding; Cellectar: Research Funding; BMS: Research Funding; Medimmune: Research Funding; Phosplatin: Research Funding; Amgen: Research Funding; Celgene: Honoraria; Janssen: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal